

Can I Leave Two Tendons Without Repair In My Shoulder
Frequently Asked Questions
Why am I still having symptoms after rotator cuff surgery?
The virtually common causes of pain after rotator cuff surgery are (1) that the shoulder is all the same recovering from the surgery itself and (2) the shoulder has gotten stiff due to lack of movement. It is well known that rotator cuff surgery is a major performance where the rotator gage tendons (Figure 1) are sewn back to the upper arm os (humerus) (Figures 2 and three).
The other major reason patients have hurting after rotator cuff surgery is due to stiffness of that shoulder. It is common afterward rotator cuff surgery to take some stiffness due to the fact that the operation caused the arm to exist held without motion for some fourth dimension. It is of import after the surgery to protect the rotator cuff repair for several weeks while it heals, and during this time it is very mutual for the shoulder to get strong to a lesser or greater degree. Your doctor and physical therapist tin can keep an heart on this for you lot and permit y'all know if your stiffness is the expected corporeality or too excessive. Often times the stiffness can be treated, and the hurting resolves.
It takes the repaired rotator cuff tendons about six weeks to heal initially to the bone, 3 months to form a relatively strong zipper to the os, and about 6 to nine months before the tendon is completely healed to the bone. Nearly patients who have had rotator cuff surgery will tell y'all that information technology takes most 9 months before the shoulder feels completely normal. This observation is supported by a report showing that in patients who accept had rotator cuff surgery, strength in the shoulder muscles is not fully recovered until nine months after the surgery. As a result, it is normal to wait some connected symptoms of pain or soreness subsequently rotator gage surgery for several months.
How do I treat the stiffness?
You lot should always follow the directions of your surgeon after surgery, since some tears need more time to heal than other tears. The all-time affair is to heed to your md as well as the physical therapist involved in your intendance. We tell our patients that ice is helpful for the pain, forth with pain medicine of some sort, such equally acetaminophen (east.chiliad. Tylenol), anti-inflammatory medications (e.grand. aspirin, ibuprofen, naproxen, etc.), pain relievers (non-narcotic or narcotic) and even prednisone by rima oris (e.g. cortisone dose packs). Yous should take these medications only at the direction of your doctor. We usually recommend that during the first iii months the emphasis in physical therapy and with your dwelling house plan should be on regaining motion in your fingers, wrist, elbow and shoulder. Nosotros tell patients they have the rest of their lives to get strong, just during the start 4 months subsequently rotator cuff surgery, the major goal should be largely to regain motion in the shoulder. Stiffness in the shoulder tin can be the cause of pain months after the surgical repair, so it is important that stiffness exist addressed fifty-fifty months or years after the surgery.
How much therapy should I take after surgery?
Your surgeon can answer this since they are the ones who know how much work had to exist washed to repair the tendons. The doctors tin can prescribe therapy based on the work done during the operation. If more than one tendon had to be repaired or if the tendon tear is a large tear, the surgeon may recommend that the therapy progress slower to allow more time for healing; on the other hand, if the tear is small, they may allow a piddling more motion before than usual subsequently the surgery.
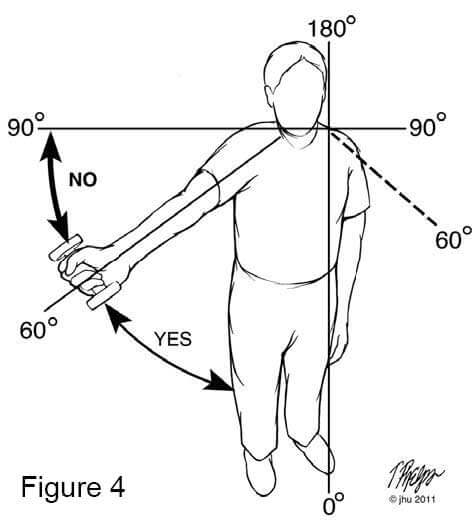
It is possible to have as well much therapy, and that is usually experienced as lots of hurting afterwards the therapy session or hurting for days after the therapy session. It is of import that the concrete therapist has a dialogue with you to make sure that the exercises are done at a proper pace for your particular surgery. We typically recommend concrete therapy only twice a week. All the same, nosotros recommend that patients stretch on their own the other days when they do not see the therapist. Sometimes physical therapy with the therapist three times a calendar week is indicated, and this should be discussed with your md and physical therapist. Similarly, it is typically not necessary to stretch more than one time or at almost twice a twenty-four hours with a home programme. Lastly, if strengthening exercises are causing y'all pain, we recommend that you do not do the exercises over 60 degrees of superlative of the shoulder (Effigy 4). This is because the rotator cuff begins to have increased stress above this level, and it can worsen the pain if the shoulder is irritated already. We recommend that y'all water ice the shoulder after any do programme to continue the pain under control.
What if I feel a tear or pull in therapy?
It is not uncommon to have a small-scale "twinge" or "pull" in physical therapy, which typically does not mean that the rotator cuff repair has failed. Normally these small twinges are unremarkably nothing to worry near. Information technology is non really known what causes them, but it is believed that information technology may be scar tissue existence stretched or the shoulder joint moving effectually normally in the socket. It would be rare for the therapy to really cause a repaired tendon to tear, as volition be discussed later.
How practice I know if the tendon repair has torn again?
It is not easy to tell if the rotator cuff tendon repair has failed or not. The symptoms of pain or loss of strength are common afterwards rotator cuff surgery while the tendons are healing, and minor setback are to exist expected. We practice not recommend a magnetic resonance browse or other studies when these setbacks occur for several reasons. The outset reason is that magnetic resonance imaging after a surgical repair of the rotator gage does not have the same accuracy in determining whether tendons are torn. If an MRI is performed, we recommend that it exist performed with dye in the afflicted shoulder (arthrogram) with a needle under x-ray or CAT scan guidance by a radiologist. This test is called an arthrogram-MRI and may exist positive if the tendon has non had plenty time to heal or if parts of the tendon have not healed to os. Equally a result, within three months after a rotator cuff repair, it is common for the dye to leak through the tendon since it has not completely healed. After this period of time, the degree of tear in the tendons can be adamant all-time with this report.
What practise I practise if my tendon has not healed?
The reality of rotator cuff surgery is that while well-nigh tendons heal dorsum to the bone after surgery, not all repaired tendons heal completely, and some do not heal at all. There are many reasons for this lack of healing with surgery. The outset is that the rotator cuff tendons are large tendons which may have also extensive harm to heal. The rotator gage tendons are large, and there are iv of them. Each rotator cuff tendon is as thick as your pinkie and equally wide every bit ii to three fingers. The chance that the tendons will heal with surgery is directly related to how large the tear in the tendons was before surgery. How to determine the size of the rotator gage tendon tear will be discussed below.
The 2nd reason that the tendons may not have healed with surgery is that these tendons begin to wear out in most humans showtime around the age of 30, and the corporeality of vesture and tear varies from person to person for reasons we do non empathise. This article of clothing of the tendons occurs in some people but not in others. By the age of 50, many people take some article of clothing of their rotator cuff tendons.
When rotator gage tendons tear prior to any surgery, in that location are two ways they can tear. The first is that there is an injury that pulls the tendon off the bone. When this happens, there is still some tendon left to repair with very little tendon missing. Still, in many cases when the tendon tears with minimal trauma, the reason the tendon tore in the outset place was because it already had some trigger-happy due to wear and tear over the years. This wear and tear over time is the second manner the tendon tin can tear. This type of tear is best described as a tear that occurs in a way analogous to "wearing a hole in the seat of ane'south pants"; the tendon just gets thinner and thinner over time until at that place is a hole there (called an "attritional tear"). This type of rotator cuff tendon tear typically happens without the person being aware that information technology is happening.
The affair that is strange virtually this type of rotator cuff tear is that they can occur and not crusade whatever problems until the tear gets big. These "habiliment a hole in your pants" tears can be any size from the size of a pinhole to "massive" tears where there is little tendon left. In these tears, the edge of the tendon at the hole is thin, and information technology is difficult to sew together it back together. If 1 tries to repair a pigsty in the tendon that is the size of ane fingernail or smaller, information technology is easier to repair than a larger hole. In large holes caused by this blazon of damage (attritional or "wear a hole in your pants" type of tear), the rotator gage tissue around the edges is not equally sturdy, and 1 is asking the tissue to fill a hole where in that location is really no tendon. For this reason, the major factor in determining whether a rotator gage tear tin can heal is how big the pigsty was to being with prior to the surgery. The larger the rotator cuff tear before surgery then the college the failure charge per unit of surgery.
How exercise you describe the size of tendon tears?
The showtime way to describe tears of the rotator cuff tendons is whether tears are part of the way through (called "partial thickness") or all the mode through the tendon (chosen "full thickness". The tears of the rotator gage tendons can exist fractional thickness (similar sawing through a rope part of the way) (Figure 5) or they can progress to tears all the fashion through the tendon (like sawing all the manner through a rope) (Figure 2). One time a tear is all the manner through the tendon (chosen "full thickness"), the next result to consider is the size of the pigsty in the tendon. Every bit the tendons tear more, they tin can exist of any size (depth and width).
The normal anatomy of the shoulder and rotator gage tendons are demonstrated in Figure vi. Full thickness tears of the rotator cuff are described as small, medium, big or massive (Figures 7, 8, 9 and 10). Since well-nigh rotator gage tendons are virtually as wide every bit three of your fingers, a small tear would be i the size of your fingernail or smaller (less than one centimeter of tendon torn) (Figure vii). A moderate size full thickness tear through the tendon would exist one that is the size of three fingernails (nearly one centimeter in i direction and three centimeters in another). Usually tears of this size mean the whole tendon width is pulled off of the bone (Figure 8). A large tear is i that would hateful the tendon is torn from the knuckle to your fingertip; this is chosen a large or massive tear (Figures 9 and 10). It is also possible to tear more than one tendon completely. The size of the tear is very important every bit it determines the chances that the tendon will heal with surgery.
What are the chances a tear will heal with surgery?
In that location have been many studies that tell us approximate odds of tendons healing with surgery depend upon the size of the tendon [1, 3, 7, 13]. It has been demonstrated that pocket-sized full thickness tears the size of a fingernail (one centimeter) (Figure vii) heal in a majority of cases, only approximately 5% volition not heal for the reasons mentioned in the discussion above. For full thickness tears that are moderate size (one to three centimeters), the re-tear charge per unit is around 20% (Figure eight). For large tears (iii by v centimeters), the re-tear charge per unit is approximately 27% (Figure nine). For massive tears (where one tendon is largely or completely gone or more than one tendon is torn), the re-tear rate is anywhere from 50 to xc% [8, 14] (Figure 10). The reason for this loftier failure rate with large to massive tears is because there is a pigsty besides large to be filled by stretching the remaining tendon, and the edges of the tendon will not concord the stitches used in the repair of the tendons.
So what do I do if a rotator cuff tear fails?
Commonly a tendon repair fails because it was going to fail and not considering of a bad surgery or bad therapy. The reality is that rotator cuff surgery is not perfect, and non all tendons will heal completely with surgery. In one case a tendon has failed an attempted surgical repair, the odds are that it volition be difficult to repair once more and to get it to heal. In some cases, the tear may exist small plenty after a failed repair to be successfully repaired, merely the exact run a risk of failure with further surgery is related to how big the tear is at that time. The larger the tear, the less likely it can be successfully repaired a 2nd fourth dimension. In most cases a 2nd attempt at repairing the tendon is not going to be successful unless the tear is small-scale.
If the tendon has re-torn and cannot exist repaired with further surgery, there is still hope for the function of the shoulder; the shoulder is not doomed and all is not lost. In that location are two myths virtually rotator cuff tears. Ane myth about rotator gage tears is that the shoulder is doomed if the tendon is not repaired. The reality is that some people can have good range of motion and function with torn rotator cuff tendons. The caste of symptoms subsequently a failed rotator cuff repair depends upon many factors. The typical symptoms of shoulders with un-repaired tendon tears are weakness with lifting above shoulder level or away from the body. The symptoms can often be controlled by watching one's activities, maintaining a good range of motion of the shoulder, and being careful about how much lifting one does with the shoulder. Basically one can exercise any activity he/she chooses every bit long as information technology does not hurt. We recommend that the patient lets their symptoms be their guide to activity level.
The second myth about have a rotator cuff tear that is too large to repair is that the shoulder is doomed to go arthritis or to gradually lose function. There is no manner to predict what rate the shoulder will accept any bug or if it will take whatever problems at all. At that place is but one report which has suggested that the shoulder with no rotator gage tendons may develop arthritis over time [10]. This study was non conclusive, then information technology is currently believed that being active does not lead to degeneration of the shoulder when there are irreparable tears. We encourage people with torn rotator cuff tendons that cannot be repaired to be as active equally possible within the limits of their pain and weakness.
What about patching up the hole?
For decades in that location have been many attempts at finding some tissue or something manufactured to put in the hole of the torn rotator gage tendon to help it heal. Unfortunately most of those attempts take failed every bit they do not regenerate or heal the pigsty in the rotator cuff tendons. Things that have been used unsuccessfully to patch the hole in the by include a person's ain tissue (called "autografts" and include iliotibial ring and biceps tendon), a cadaver or human donor tissue (called "allografts" and include iliotibial band and posterior tibialis tendons from the leg), tissue from animals (called "xenografts" and include sterilized pig-gut mucosa) and more recently patches made from culture cells (human skin cells, fibroblast scaffolds). In most instances these accept no restored function and strength to the shoulder, and they should be considered experimental at this time. We exercise not recommend them in most instances, especially in tendon tears that have had previous surgery that has failed. Some physicians recommend these patches in tears that are very large, but the failure rate is exceedingly high. There is currently no known or proven advantage to using patches in the repair of torn rotator cuff tendons.
What about tendon transfers?
A tendon transfer is an operation where the tendon of another muscle around the shoulder is moved to replace the rotator gage tendon. There are a couple of tendon transfers that have been described for this purpose [ii, nine, 11]. The outset is a large muscle in the dorsum of the shoulder called the "latissimus dorsi muscle." While this is a large musculus, the tendon is actually very thin and non very big. While this operation was once advocated for patients with large rotator cuff tears with pain, the results were non as skillful as initially reported. This operation is helpful for simply a minority of patients and has lost favor among shoulder surgeons [12].
A 2nd muscle and tendon transfer that was described once was the employ of the deltoid muscle and tendon as a buffer or spacer for the space where the rotator cuff tendons were located. This operation was largely a failure and is no longer recommended.
What about shoulder replacement?
Shoulder replacements for patients with rotator cuff tears can exist successful but patient eligibility continues to modify and evolve. Typically shoulder replacements are reserved for patients with torn rotator cuffs who also accept arthritis of the shoulder articulation. The replacements are not often used for patients who have just loss of motion lonely, and we tell patients that the replacements are indicated mainly for reducing pain in the shoulder. However, equally there are increasing improvements in shoulder replacements, this may change and should be discussed with your dr..
In that location are several kinds of shoulder replacements bachelor for patients with arthritis and painful rotator cuff tears. Each blazon has its advantages and disadvantages depending on the historic period of the patient, the activeness level of the person, and the corporeality of damage to the shoulder. In some instances information technology might be best to supersede the shoulder with a more than conventional shoulder replacement. A relatively new prosthesis called the reverse prosthesis has had some promise in patients with arthritis and torn rotator cuff tendons that are non repairable. These operations are generally very good for pain relief and do result in some improvements of motion. The pluses and minuses of these procedures should be discussed with your dr..
References
- DeOrio, J.G. and R.H. Cofield, Results of a 2nd endeavor at surgical repair of a failed initial rotator-cuff repair. J Bone Joint Surg Am, 1984. 66(4): p. 563-7.
- Chaffai, M.A. and M. Mansat, Anatomic basis for the construction of a musculotendinous flap derived from the pectoralis major muscle. Surg Radiol Anat, 1988. ten(four): p. 273-82.
- Harryman, D.T., 2nd, et al., Repairs of the rotator cuff. Correlation of functional results with integrity of the cuff. J Bone Joint Surg Am, 1991. 73(vii): p. 982-ix.
- Rokito, A.S., et al., Strength after surgical repair or the rotator cuff. J Shoulder Elbow Surg, 1996. 5(one): p. 12-7.
- Rokito, A.S., et al., Long-term functional upshot of repair of large and massive chronic tears of the rotator gage. J Bone Joint Surg Am, 1999. 81(vii): p. 991-7.
- Davidson, P.A. and D.Westward. Rivenburgh, Rotator cuff repair tensions as a determinant of functional issue. Journal of Shoulder and Elbow Surgery, 2000. 9(6): p. 502-506.
- Jost, B., et al., Clinical outcome afterwards structural failure of rotator cuff repairs. J Bone Joint Surg Am, 2000. 82(3): p. 304-xiv.
- Motamedi, A.R., et al., Accuracy of magnetic resonance imaging in determining the presence and size of recurrent rotator cuff tears. J Shoulder Elbow Surg, 2002. 11(one): p. 6-10.
- Iannotti, J.P., et al., Latissimus dorsi tendon transfers for irreparable posterosuperior rotator cuff tears. Factors affecting outcome. J Bone Joint Surg Am, 2006. 88(2): p. 342-eight.
- Zingg, P.O., et al., Clinical and structural outcomes of nonoperative management of massive rotator cuff tears. J Bone Joint Surg Am, 2007. 89(9): p. 1928-34
- Derwin, Grand.A., et al., Rotator gage repair augmentation in a canine model with use of a woven poly-L-lactide device. J Bone Joint Surg Am, 2009. 91(five): p. 1159-71.
- Nove-Josserand, L., et al., Results of latissimus dorsi tendon transfer for irreparable cuff tears. Orthop Traumatol Surg Res, 2009. 95(2): p. 108-13.
- Slabaugh, M.A., et al., Does the literature ostend superior clinical results in radiographically healed rotator cuffs later on rotator gage repair? Arthroscopy, 2010. 26(three): p. 393-403.
- Kluger, R., et al., Long-term Survivorship of Rotator Cuff Repairs Using Ultrasound and Magnetic Resonance Imaging Analysis. Am J Sports Med, 2011.

Source: https://www.hopkinsmedicine.org/orthopaedic-surgery/specialty-areas/shoulder/treatments-procedures/failed-rotator-cuff-repairs.html
Posted by: mayonstent1991.blogspot.com
0 Response to "Can I Leave Two Tendons Without Repair In My Shoulder"
Post a Comment